

Emirates Flight 131 – How an accident was averted
Emirates Flight EK131 - How an accident was averted
Overview
What Happened
The report, published in April 2020 by the United Arab Emirates General Civil Aviation Authority, examined the event in detail. It presented a picture of human-machine interface breakdown, less than ideal communication, and shortcomings in training.
But communication soon broke down. From the report: The Investigation believes that their shared mental model of ‘becoming high on profile’ started to diverge when the commander suggested requesting a descent to 500 metres QFE, as a prevention strategy to avoid being high on profile. (Altitudes below flight level transition altitude are given in metres in Russia). This, probably, happened since the commander did not call this out or explain to the co-pilot the intent of his suggestion, which was to prevent the aircraft from becoming high on profile.
How did it happen?
The first officer did not realise that the descent to 500 meters would place the aircraft on the correct vertical profile. Thinking they were still high, he attempted to intercept the glideslope from above, as per the procedure.
The report mentions ‘confirmation bias, which resulted in testing his beliefs or hypothesis in a one-sided way by only searching for evidence or information that supported his belief.’
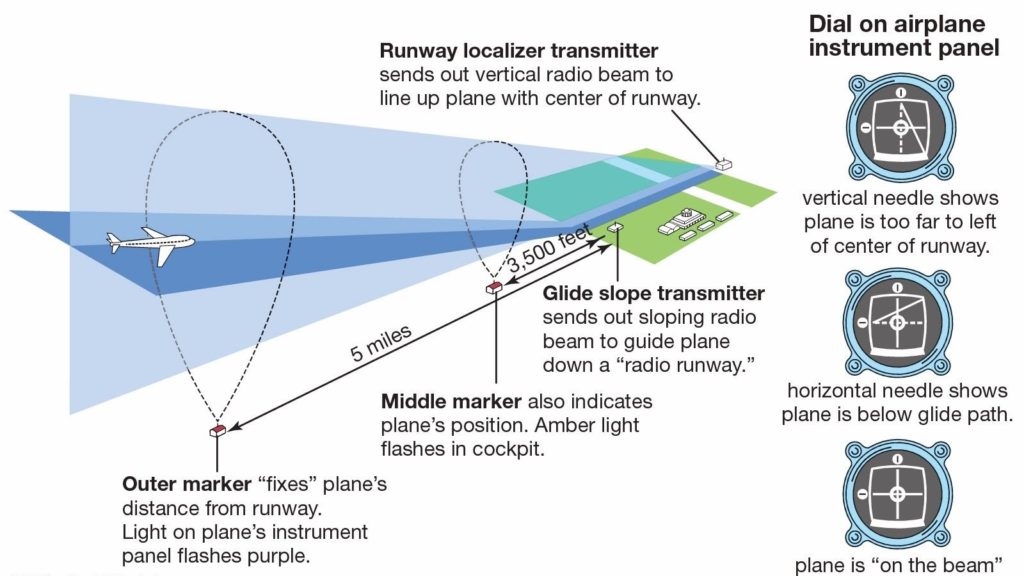
The first officer was watching the glideslope indicator, but its deviation information was invalid because the aircraft position was outside the azimuthal (side-to-side) coverage of the ILS glideslope signal. See the image at the end of the post to see a typical ILS azimuth and glideslope coverage. When the aircraft came within the glideslope signal’s azimuthal coverage, it had descended so much that it was outside the elevation coverage. The report notes the first officer could have cross-checked the indicator against pressure altitude, vertical and navigation displays, and the DME distance table in the approach chart, a technique which is called checking RAW DATA, but he did not do so.





Meanwhile, the aircraft continued to descend. There was no action by either flight crew member to stop the aircraft from descending. The radar controller called with a lengthy (17 seconds) instruction in non-standard phraseology ‘not to descend further’. Several seconds later, at 504 feet, the crew began a go-around. The A380’s considerable inertia ‘mushed’ it down to 395 feet AGL before climbing away.
As they prepared for the second approach, in accordance with standard operating procedures, a multi-waypoint sequencing in a row of the flight plan occurred at a location where several waypoints satisfied the FMS’s geometrical waypoint sequencing rules. This caused the automatic reset of the captain’s FMS and the flight plan disappeared from the flight management system (FMS) leaving a blank screen. At the point when the commander chose the runway waypoint utilizing the ‘direct to’ mode on the FMS. The aircraft leveled off at 2600 feet QNH and they came in for a third approach.
Why did it happen?
Rather than condemn the crew’s human factors, situational awareness and human-machine interface performance, the report put them into context.
It quoted Key Dismukes, a NASA human factors expert, and Ben Berman (authors of the 2007 book, The Limits of Expertise: Rethinking Pilot Error and the Causes of Airline Accidents) (CLICK HERE to buy or go to the image link below) who wrote in a 2010 paper:

Even though automation has enhanced situation awareness in some ways, such as navigation displays, it has undercut situation awareness by moving pilots from direct, continuous control of the aircraft to managing and monitoring systems, a role for which pilots are poorly suited.
Closer Examination is expected to create simple human strategies to assist pilots to remain tuned in on present airplane status, configuration, flight path monitoring, and energy management. The job of the Pilot Monitoring (PM) needs to be defined better and intervention strategies planned to find ways to make it easier.
These new structures must be instinctive, easy to adapt, and evoke a favorable response. This will empower the pilot monitoring those who are flying and potentially making mistakes to be attentive, amongst the numerous other attentional requests of dealing with the flight.

The incident report also noted the Flight Safety Foundation’s four reasons why monitoring is difficult for pilots:
- the human brain has difficulty with sustained vigilance
- the human brain has quite limited ability to multitask
- humans are vulnerable to interruptions and distractions
- humans are vulnerable to cognitive limitations that affect what they notice and do not notice.
As an internal mechanism to deal with the incident, Emirates reviewed its procedure for intercepting the glideslope from above. It published a flight safety update that discussed the problems of using ILS outside its certified envelope. It also incorporated the tale of flight EK131 into recurrent training for its crews.


